Home / A Case Against Water Fluoridation – Scotland

The National bird of Scotland is the
Golden Eagle. – Aquila chrysaetos.
 Since the early trials, more than 60 years ago
Since the early trials, more than 60 years ago
the incidence of caries has declined similarly
in fluoridated & non-fluoridated communities!

RECOMMENDED READING

The Scottish Dental Magazine is the essential
magazine for dental professionals in Scotland.
◊ ◊ ◊
A Case Against Water Fluoridation
‘Safe and effective’ has long been the mantra of proponents of water fluoridation. To be clear at the outset, I am not discussing here the use of topical fluoride (as in toothpaste, rinses etc), but questioning the mantra over the efficacy, safety – and also propriety – of adding fluoride to the public water supply.
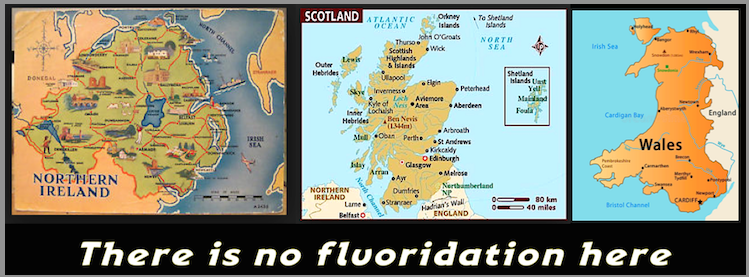
In line with nearly all of Europe and most other countries, we do not fluoridate our water in Scotland, relying instead on the forward-looking Childsmile programme. But occasional voices still call for its reintroduction and it is worth considering how inadvisable such a retrograde step would be.
.
Does it work?
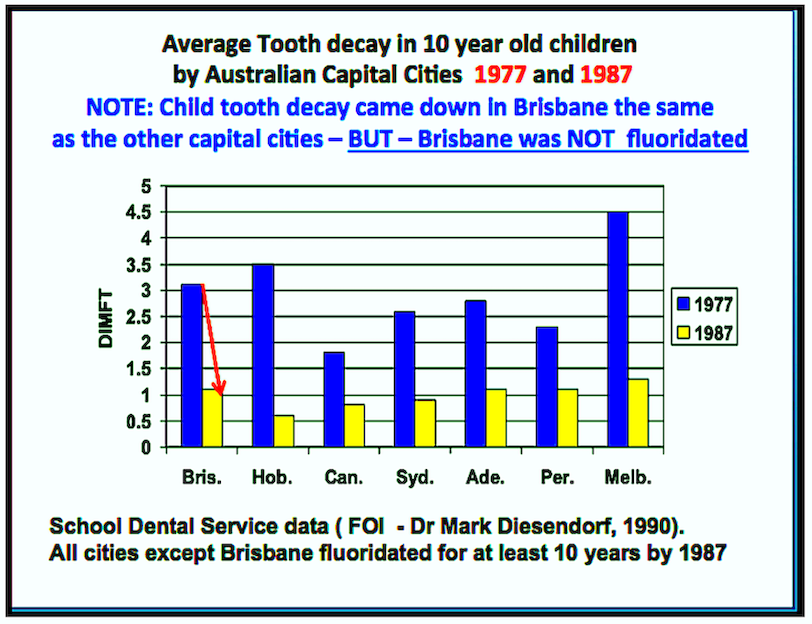
Since the early trials, more than 60 years ago, the incidence of caries has declined similarly in fluoridated and non-fluoridated communities -2, probably due in part to fluoride toothpaste and, in part, to better diet and living conditions. Today, fluoridation may still have some effect, but it is marginal and less than has often been claimed.
Such a lukewarm endorsement may seem surprising when one considers how energetically the practice has been promoted, even described by the US Centers for Disease Control as ‘one of the great public health achievements of the twentieth century’. But any benefit of fluoride is now agreed to be primarily topical and does not, as was long believed, involve incorporation into the enamel of the developing teeth (which results in fluorosis, see below).
Thus it does not need to be swallowed. While salivary fluoride is often believed to play a role in caries control, it appears that the concentration of fluoride in ductal saliva is too low to exert a significant effect, the residue from toothpaste being a more important source -3,4.
None of the largest trials conducted since the 1980s has demonstrated more than an almost trivial effect. That has not usually been apparent from the abstracts of the reports, which talk about impressive-sounding reductions in caries of 25 per cent or more. But the use of relative percentage changes can be very misleading when small numbers are involved. For example, a 25 per cent reduction reported for 12 year olds in 1990 -5 turned out to represent just one-sixth of a tooth surface, an absolute reduction of less than 1 per cent.
Moreover, even that small reduction is really only a delay: the number of DMF teeth increases during the teens almost equally in fluoridated and non-fluoridated areas with the former lagging the latter by a few months.
This may simply be due to a delay in the eruption of the permanent teeth –6.
An even smaller effect was seen in Australia -7. A recent survey using registry data from Denmark -8 provides a curious exception, describing an anti-caries effect of even very low concentrations (0.125-0.25 mg/l) of naturally occurring fluoride in drinking water, even where fluoride toothpaste is generally used.
Vitamin D status could be a possible confounding factor here, since it happens that areas of high natural fluoride levels in the east of Denmark also tend to receive higher levels of UV-B irradiation -9, but further investigation is needed. Reports from Finland, the former East Germany and Cuba -10-12 show that when fluoridation ceased, caries rates in children remained static or declined. This may have been partly due to the use of topical fluoride applications, but the important point is that fluoridation was clearly shown to be either ineffective or easily replaceable.
Although it is widely believed that fluoridation is particularly beneficial to poorer communities, the York -13 and European Commission SCHER -14 reports considered that the evidence supporting such a selective benefit was fairly weak. It has been described with some reason as a ‘sticking plaster’ measure to avoid dealing with inequalities in a more fundamental way. Awofeso -15 has recently argued cogently that fluoridation cannot be justified ethically on the grounds of its public value. Cheng et al2 also provide a useful discussion of this issue.
.
What are the risks?
Numerous government agencies in the main fluoridating countries – USA, Australia, New Zealand, Irish Republic – have continued to assert the safety of fluoridation since its original endorsement by the US Public Health Service in 1950. Such assurances rest more on faith than reality since very few studies have, in fact, been done to investigate the range of plausible dangers identified in animal or biochemical studies or the prolific anecdotal evidence that some people are hypersensitive to fluoride. So, health authorities can continue to state that there is ‘no evidence’ of harm. The oft-repeated belief that ‘if there was any danger we’d have noticed it by now’ is not well founded.
There are many sources of fluoride exposure, so even if the fluoride imbibed with water alone is not enough on its own to cause harm, its presence may tip the scales. Mansfield -16 has calculated that many people in the UK are exceeding the total intake of fluoride that is officially recognised as safe, and the proportion is higher in fluoridated areas.
.
Dental fluorosis
This is the one risk that everyone agrees about – usually (not always) very mild or mild, but readily visible particularly on the maxillary incisors, and not always appreciated by the owner. More important than any cosmetic effect are the underlying mechanisms, including disruption of normal mineralisation by the incorporation of fluoride into apatite crystals producing fluorapatite and interference with the function of ameloblasts17 with resulting irregularities in the mineral structure. The teeth provide a visible window to the largely hidden effects that these processes may have on the skeleton over a lifetime.
.
Skeletal fluorosis
Throughout life, about 50 per cent of ingested fluoride accumulates in the skeleton, especially at sites of bone formation. Advanced (clinical Stage 3) skeletal fluorosis occurs in parts of India and elsewhere where fluoride is naturally present in the water at 5ppm or more – a devastating condition fortunately very rare in the west. The question mark for us hangs over the earlier clinical Stages 1 and 2, which manifest as aches and pains and later arthritis. The extent to which this may contribute to the spectrum of arthritic conditions in western countries is unknown18,19.
.
Carcinogenesis
Related to its localisation in bone, fluoridated water consumption specifically between the ages of five and eight has been implicated in the development of osteosarcoma in young men -20. This was a carefully conducted case-control study that confirmed tentative suggestions from some earlier cross-sectional studies.
Although ecological studies have mostly failed to detect an association between osteosarcoma and fluoridation, that may well be due to the rarity of the disease and the relative weakness of cross-sectional investigations. So far there have not been any attempts to repeat Bassin’s work, or any convincing evidence to suggest that its conclusions were wrong, so it remains both biologically plausible and unrefuted.
Fluoride has also been claimed to be a more general carcinogen, but the evidence remains unconvincing. However, the silicofluorides commonly used for fluoridation are contaminated with arsenic.
A typical (USA) concentration of 30mg As per kg of silicofluoride would be expected, assuming a linear carcinogenic dose-response relationship, to result in 2.7 extra cases of lung and bladder cancers per million people drinking the fluoridated water -21.
.
Thyroid and other organs
Fluoride interferes with the activity of a large number of enzymes in vitro. Animal studies have indicated low-dose toxicity of fluoride to several organs and systems including the kidneys and particularly the thyroid -18. It is considered to be an endocrine disruptor 18. There is as yet no compelling evidence that dietary fluoride intake can affect these organs in humans, but the possibility has received scant research attention and urgently
requires more.
.
Brain and IQ
One topic that is receiving considerable attention at present is the developing brain and IQ. There are numerous animal studies documenting damage to the brain, especially during development. One important mechanism is interference with enzymes such as superoxide dismutase and catalase that protect metabolically active cells and tissues against oxidative damage -22.
Reductions in children’s IQ have come to prominence as a result of more than 30 studies conducted in regions of China and elsewhere that have naturally high concentrations of fluoride in the drinking water. A systematic review and meta-analysis from Harvard of 27 studies 23 concluded that, although most had shortcomings and dealt with higher fluoride concentrations (most in the range 1-5ppm) than used for fluoridation (0.7-1.0ppm), there was almost universal agreement that higher fluoride led to lower IQ.
The average reduction over the series was seven IQ points, [for each generation]. At best, this implies a margin of safety that is extremely low by normal toxicological standards.
Proponents of fluoridation have been quick to denigrate and downplay these studies, but despite some weaknesses in the individual studies – some inherent in the type of epidemiological design used – the consistency of the results demands attention. While they do not directly implicate artificially fluoridated water at 0.7-1.0 mg/l, the risk is clearly there and, as the review authors say, requires further research.
.
Is it ethical?
Our right as individuals to refuse medication is enshrined in law though whether that right is absolute or conditional – on, for example, an estimate of a public good such as the care of poor children 2,15 – is disputed. Proponents argue that fluoride is not a medicine, but a natural mineral nutrient, like calcium, that is simply supplemented to an ‘optimal’ concentration.
The fact that it is ‘natural’ carries no weight: arsenic is natural too. Nor is it in any way comparable to calcium, an essential nutrient, or even to selenium, which despite being highly toxic is still essential in trace quantities; fluoride is not required for any physiological process at all. It is not a nutrient, but a medicine, delivered without individual consent.
Moreover, it is delivered in a most incompetent manner, since the so-called optimal concentration is a statistical compromise and tells us little about the dosage to an individual consumer – an essential consideration for any prescribed medicine.
Young children are particularly likely to receive an excessively high dosage -14,19.
Fluoride’s medicinal status is confirmed legally by Lord Jauncey’s opinion: “
Section 130 [of the Medicines Act 1968] defines ‘medicinal product’ and I am satisfied that fluoride in whatever form it is ultimately purchased by the respondents falls within the definition.” 24
Shaw 25 argues that fluoridation in the UK subsists on the assumption that fluoride is not a medicine and that the assumption is a ‘legal fiction’.
.
Conclusion
The precautionary principle calls for risks not to be taken unless more than balanced by countervailing benefits. If there is one situation where the principle should be invoked, it is surely the involuntary mass-medication of a population with largely uncontrolled dosages via the public water supply.
The risks of water fluoridation are substantial and varied, if still mostly unproven, and the benefits today are marginal. People should not be medicated without consent. Ineffectiveness, safety concerns and ethics all point in the same direction: we are better off without it.
About the author
H S Micklem is an emeritus professor in the School of Biological Sciences, University of Edinburgh. He holds MA and DPhil degrees from the University of Oxford. He is co-author of The Case Against Fluoride (Chelsea Green Publishers) xvi+372pp 2010.
References:
2.) Cheng K K 2007. Adding fluoride to water supplies. BMJ 335,699-702
3.) Centers for Disease Control and Prevention 2001. Recommendations for using fluoride to prevent and control dental caries in the United States. Morbidity and Mortality Weekly Reports 50, RR-14, 3 http://stacks.cdc.gov/view/cdc/7086/
4.) Lambrou D et al 1981. The effect of fluoride in saliva on remineralization of dental enamel in humans. Caries Res. 15(5):341-5.
5.) Brunelle JA, CarlosJP 1990. Recent trends in dental caries in U.S. children and the effect of water fluoridation. Journal of Dental Research 69, Special Issue, 723-727
6.) Komarek A 2005. A Bayesian analysis of multivariate doubly-interval-censored dental data, Biostatistics 6(1). 145-155
7.) Spencer AJ et al 1996. Community fluoridation in Australia. Community Dental Health 13, Suppl 2, 27-37.
8.) Kirkeskov L et al 2010. The association between fluoride in drinking water and dental caries in Danish children. Linking data from health registers, environmental registers and administrative registers. Community Dent Oral Epidemiol 38, 206-2012.
10.) Seppä L et al 2000. Caries in the primary dentition, after discontinuation of water fluoridation, among children receiving comprehensive dental care. Community Dent Oral Epidemiol. 28, 281-8.
11.) Kunzel W et al 2000. Decline of caries prevalence after the cessation of water fluoridation in the former East Germany. Community Dent Oral Epidemiol 28, 382–9.
12.) Kunzel W, Fischer T 2000. Caries prevalence after cessation of water fluoridation in La Salud, Cuba. Caries Res 34, 20-25.
13.) McDonagh M et al. 2000. A systematic review of public water fluoridation, NHS Centre for Reviews and Dissemination. http://www.york.ac.uk/inst/crd/CRD_Reports/crdreport18.pdf
14.) Scientific Committee on Health and Environmental Risks (SCHER) 2011.Critical Review of any new evidence on the hazard profile, health effects, and human exposure to fluoride and the fluoridating agents of drinking water. http://ec.europa.eu/health/scientific_committees/environmental_risks/docs/scher_o_139.pdf
15.) Awofeso N 2012. Ethics of artificial water fluoridation in Australia. Public Health Ethics 5(2) 161-172.
16.) Mansfield P 2010. Fluoride consumption: the effect of water fluoridation. Fluoride 43(4), 223-31
17.) Bronckers ALJJ et al 2009. The impact of fluoride on ameloblasts and the mechanisms of enamel fluorosis. J Dent Res. 88(10), 877–893.
18.) National Academy of Sciences 2006. Fluoride in drinking water: a scientific review of EPA’s standards. http://www.nap.edu/catalog/11571.html
20.) Bassin EB et al 2006, Age-specific fluoride exposure in drinking water and osteosarcoma (United States). Cancer Causes Control 17, 421–428.
21.) Hirzy WJ et al 2013.Comparison of hydrofluorosilicic acid and pharmaceutical sodium fluoride as fluoridating agents – a cost-benefit analysis.. Environmental Science & Policy 29, 81-86.
22.) Madhusudhan N et al 2009. Fluoride-induced neuronal oxidative stress and its amelioration by antioxidants in developing rats. Fluoride 42(3) 179-187.
23.) Choi AL, Sun G, Zhang Y, Grandjean P 2012. Developmental fluoride toxicity: a systematic eview and meta-analysis. Environmental Health Perspectives 120(10) 1362-1368. http://www.ncbi.nlm.nih.gov/pmc/?term=10.1289/ehp.1104912
25.) Shaw D. 2012 Weeping and wailing and gnashing of teeth:
The legal fiction of water fluoridation.
Medical Law International 12(1), 11-27
.


.
Reprinted here by:


The Golden Eagle is the top
predator in the Scottish countryside.